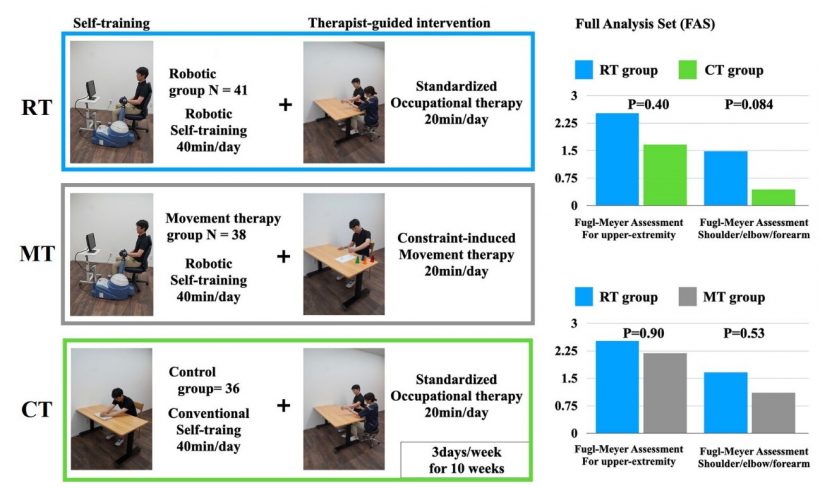
 with Fugl-Meyer Assessments (right). The Fugl-Meyer Assessment is a stroke-specific performance-based impairment index that rates patients’ ability to perform tasks on a 3-point scale, 0 indicates tasks cannot be performed, 1 partially performed, 2 performed. Credit: Osaka Metropolitan University")
One of the most common effects of strokes are hemiplegia, a partial paralysis occurring in the left or right side of the body. When it occurs in the arm or hand, it is especially devastating to a patient’s ability to perform everyday tasks. Current treatments focus on improving motor function with therapist-led stretching and exercises to strengthen muscles and improve joint mobility. Recovery is a difficult process; functionality is rarely fully restored as the benefits of rehabilitation are believed to diminish over time, leading to lingering symptoms in chronic stroke patients who remain affected 180 days post-stroke. Chronic stroke patients often struggle as medical systems typically do not have programs for continuing treatment.
A study led by Dr. Takashi Takebayashi and published in the journal Stroke suggests continuing therapy for chronic stroke patients is still beneficial while suggesting a radical alternative. Robot therapy can provide repetitive exercises while holding affected limbs, sensing force feedback, and providing real time analysis.
This led the Osaka Metropolitan University to determine if robotic therapy is as effective as traditional therapy during the chronic stage of stroke recovery. If widely adopted, robot therapy could improve care for stroke patients while being cost effective and requiring minimal therapeutic staff guidance.
The research team enlisted the help of 129 stroke patients who met screening criteria for arm and hand paralysis and provided informed consent to participate in the study. The team then coordinated efforts across 25 clinics and hospitals in Japan to test the efficacy of robot therapy. They performed a randomized controlled trial that divided patients with equally severe stroke into three groups with three one-hour weekly therapy sessions for 10 weeks, beginning six months after the patient’s stroke (Fig.1).
The control group received 40 minutes of self-training and 20 minutes of therapist-led occupational therapy, focused on traditional correct movement, joint mobility, stretching, and daily activities (Fig.1 CT). The robot therapy group began with 20 minutes of therapist-led standard occupational therapy. Followed by 40 minutes of rehabilitation with a ReoGo-J upper-limb rehabilitation device, an armature that supports the patients’ arms, senses their movement, provides feedback, and matches difficulty to the patients’ level of impairment (Fig.1 RT). The movement therapy group sought to combine 40 minutes of robot-assisted self training with 20 minutes constraint induced movement therapy (Fig.1 MT), where therapist-led exercises on hand shaping, task practice, and practice applying those skills to real life situations were conducted.
Contrary to widely accepted clinical practices, the chronic paralysis patients did show signs of improvement from the training despite being in the chronic stroke stage. Importantly, in measurements of daily tasks, the patients who received robot therapy rated the same as the control group who had therapist-led exercises.
The combined approach of robot therapy supplemented with therapist-led standardized occupational training proved most effective. This suggests not only that care for chronic stroke hemiplegia patients needs to be continued, but that robot therapy may be more influential in stroke recovery than traditional therapy alone.
The biggest differences were found in a subset of robot-therapy patients that had large improvements in shoulder, elbow, and forearm use, where the ReoGo-J upper-limb rehabilitation device program focused.
Source: Read Full Article